
TSH is often the only test performed when you get the “everything is normal” news – and this is not only incomplete, but this methodology is totally unreliable when you have Hashimoto’s.
Not to say it is not an important test, it most definitely is. TSH is a sensitive hormone that will respond to low thyroid hormone levels, it is important. It’s just that you have to know how your Hashimoto’s may affect that reading as well as the variances in the ranges of “normal” when it comes to interpreting your TSH reading.
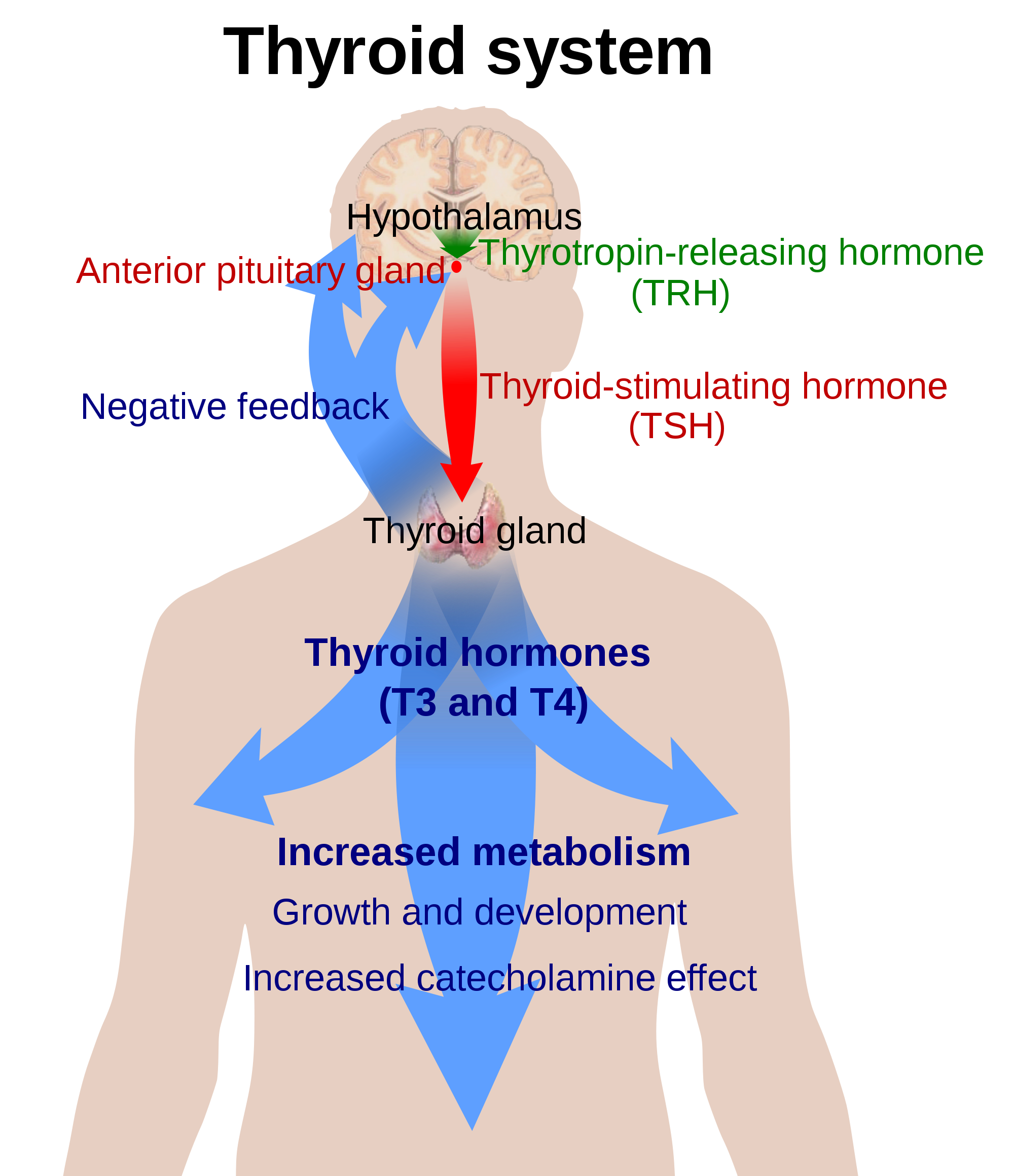
To back up a bit: TSH is the signal from your pituitary to your thyroid that says, “Hey down there, you sluggish little thyroid, make more hormone!” The hormone made then is primarily T4. TSH will rise or fall in response to lower or higher levels of T4.
This is how TSH is typically evaluated in a nutshell:
When it starts to rise docs start thinking you are hypothyroid. However, what is considered elevated is values ranging from above 5.5 for many docs, 4.5 for some and only above 3.5 for others. And an elevated TSH is often the only time any other thyroid tests are run – and we’ll get to why that’s a big problem in a minute, first back to what’s the best top end for TSH.
Most functional docs use what the 3.5 cut off as an elevated TSH, this is the value established by the Endocrine Society (https://www.endocrine.org/ . I might say we have a problem when your TSH is at 3.8 and your family practice doc would likely disagree and tell you your thyroid is “normal” or even “perfect”.
Get you FREE copy of my Guide To Lab Testing & Your Hormones
This guide covers hormonal testing and thyroid patterns and will show you how to suss out the Hormonal Dealbreakers of inflammation, anemia and blood sugar problems.
Get Your Free Lab Guide HereSo you can see where the top end of TSH is in itself a conundrum, but the bigger problem in my opinion is that TSH is just one thyroid marker – and while it’s historically been the red flag to warrant more thyroid testing, with what we know now this practice just isn’t enough.
TSH is just the signal, it doesn’t tell us how your thyroid is responding to that signal, trouble with conversion of made thyroid hormone (T4) into active thyroid hormone (T3), how much of that is free and available for action, and a host of other issues are not seen by just looking at TSH.
Take this scenario for example:
A woman with PCOS, going through perimenopause, taking the Pill or any estrogen replacement is feeling very low thyroid. When we run a full panel we see that excess estrogen is causing her thyroid binding globulin to be elevated, thus binding up too much of her free T3 (she has lower levels of free, active T3 hormone because of estrogen dominance). Her total T4 and T3 look fine because she is making enough of them and even converting T4 into active T3.
Guess what else? Her TSH is also normal (because it is low total T4 that is the signal to her pituitary to make more TSH to stimulate the thyroid and T4 value is normal in this scenario). Her only problem is with binding globulins – the protein carriers that shuttle around thyroid hormone in the blood stream. When there’s too much binding globulin it gobbles up too much free hormone and we get hypothyroid symptoms and low active, free thyroid hormone and typically with a totally normal TSH.
This is just one of the many scenarios that can create low thyroid hormone levels and low thyroid symptoms with a normal TSH. You can see where some of you suffering from low thryoid get missed right?
And How About Low TSH?
Low TSH is typically disregarded unless is it extremely low – in which case your doc will think you are hyperthyroid either due to over medication or your body somehow cranking out too much thyroid hormone (i.e. due to Grave’s Disease, primary hyperthyroidism, etc).
But what about a TSH below 1.8? Maybe around 1.0 or slightly higher? How about 0.7? These values, below 1.8 are typically considered no big deal, but it begs the question: if you don’t have loads of thyroid hormone around, why is that signal so low? Often what we see with this lowish TSH problem on labs are: TSH below 1.8 and low or low normal T4 and/or T3 and a host of hypothyroid symptoms (tired, can’t lose weight, sluggish, dressed, hair falling out, etc.)
Order Hangry right now!
If you’ve ever felt like a Hangry B*tch and are ready to balance your hormones and restore your joy in just 5 simple steps then Hangry is for you!
GET YOUR COPY NOW
Wouldn’t a better signal help you make more hormone? Yes indeed it would. Functionally low TSH (below 1.8) is typically a problem with the pituitary. This can be due to stress, inflammation or low levels or serotonin or dopamine.
Both stress and inflammation have a direct impact on the hypothalamus, yet another part of your brain involved in your thyroid health. This part of your brain tells your pituitary what to do, without it working correctly you aren’t able to make an adequate TSH signal – and women with Hashimoto’s are nothing if not stressed and inflamed, am I right?

When it comes to those brain neurochemicals, serotonin and dopamine, the neurons that feed into the pituitary from the hypothalamus need quite a lot of both of them to work correctly. This is another critical step in the end goal: enough thyroid hormone so that you don’t gain weight, feel sluggish, keep your hair, brows and lashes…and can remember where you put your keys.
So how do you know if it’s stress, inflammation or low serotonin causing your low TSH? To assess stress, it’s best to do an adrenal salivary index.
Inflammation can largely be seen with symptoms such as puffiness, joint pain, foggy brain, etc.
You can also see this in your blood work with tests such as a sed rate (known as ESR on your lab report) or hs-CRP (high sensitivity C reactive protein). These tests aren’t typically run so you’d have to ask for them to be included.
And to make matters even more unique for you women with Hashimoto’s, your TSH isn’t always stable.
Because Hashimoto’s is an autoimmune issue you are constantly battling your environment, your hormones, blood sugar ups and downs, infections, inflammation, etc., there will be intermittent times when your Hashimoto’s is “flaring up” and you can end up with a transient hyper or even just slightly hyperthyroid state. This often only lasts for a few days, but it can lower your TSH temporarily and if you got your blood drawn that day, guess what? It will be a little lower than it was the week previous.
All that to say, if you are feeling hypothyroid you need to remember these points about your TSH test:
- TSH is important but it’s only part of the story.
- Low TSH below 1.8 can indicate problems with stress, inflammation or low serotonin or dopamine and those are fixable to get you better thyroid function.
- You have to be your own best advocate here and get a full panel done.
Contact my office if you’re struggling to be heard by your doc: drbrooke@betterbydrbrooke.com
But remember, they are likely doing their very best for you, it’s just that in this case it’s simply not enough. Have more thyroid questions? I answered many of them here in these two free reports so grab these if you haven’t already: